
ფარისებრი ჯირკვლის კვანძების აღმოჩენა უმეტესად ხდება რუტინული ფიზიკური ან ინსტრუმენტული გამოკვლევების დროს.
როგორი უნდა იყოს კლინიცისტის მომდევნო ნაბიჯები, მას შემდეგ რაც დადასტურდება ფარისებრ ჯირკვალში კვანძის არსებობა?
პირველი რიგის ამოცანაა კეთილთვისებიანი კვანძების ავთვისებიანობაზე საეჭვო კვანძებისგან დიფერენცირება.
როგორც პირველ, ასევე მომდევნო ვიზიტებზე უნდა გაეცეს პასუხი სამ ძირითად შეკითხვას:
- არის თუ არა წარმოდგენილი კომპრესიის სიმპტომები, როგორიცაა დისფაგია, დისფონია ან დისპნეა?
- ცვლის თუ არა კვანძი ფარისებრი ჯირკვლის ფუნქციას? კვანძის გამოკვლევა იწყება TSH -ის განსაზღვრით.
- არის თუ არა კვანძის კლინიკა ავთვისებიანობის მანიშნებელი? მიუხედავად იმისა, რომ ფარისებრი ჯირკვლის კვანძების აბსოლუტური უმრავლესობა კეთილთვისებიანია, 5-10%-ში დგინდება მისი ავთვისებიანობა.
ფარისებრი ჯირკვლის და ირგვლივმდებარე კისრის სტრუქტურების ულტრასონოგრაფია მნიშვნელოვანი ინსტრუმენტია კეთილთვისებიანი კვანძის მალიგნიზაციის მაღალი რისკის მქონე კვანძისგან დიფერენცირებისთვის. ამ პროცესში კარგი გზამკვლევია American Thyroid Association (ATA) და American College of Radiology Thyroid Image Reporting and Data System (ACR TI-RADS) -ის გაიდლაინები.
ულტრასონოგრაფიული სურათის მიხედვით ATA-ის გაიდლაინი ფარისებრი ჯირკვლის კვანძებს აჯგუფებს, როგორც: კეთილთვისებიანი, ძალიან მცირე რისკის, მცირე რისკის, ზომიერი რისკის და მაღალი რისკის კვანძებს.
კეთილთვისებიანი კვანძების კატეგორიაში შედის სრულად ცისტური კვანძები ქსოვილოვანი კომპონენტის გარეშე. ასეთი კვანძების მალიგნიზაციის რისკი 1%-ზე დაბალია და მისი მონიტორინგი შესაძლებელია გაგრძელდეს ბიოფსიის გარეშე. შესაბამისი ჩვენების არსებობის შემთხვევაში, შესაძლებელია გაკეთდეს დიდი ზომის სიმპტომური ცისტების დრენაჟი.
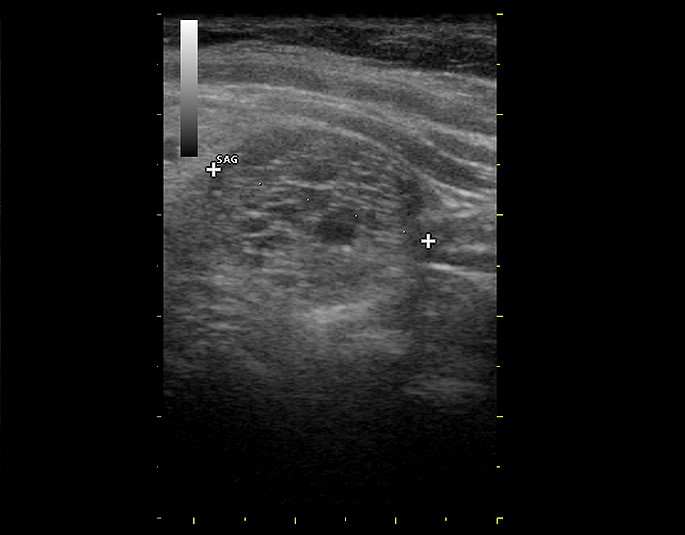
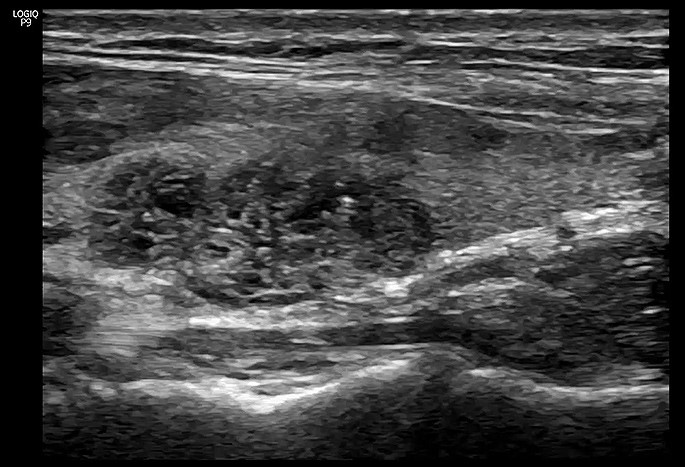
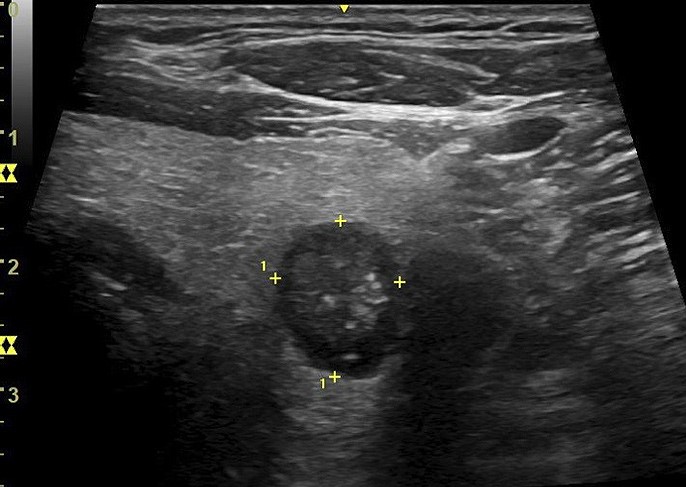
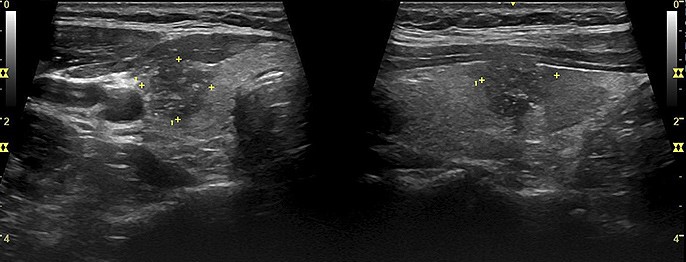
ძალიან მცირე რისკის კვანძების კატეგორიაშია ღრუბლისებრი შენების კვანძები (კვანძის >50% შედგება მიკროცისტური სივრცეებისგან) და ნაწილობრივ ცისტური კვანძები, რომელსაც არ აღენიშნება მალიგნიზაციის მაღალი რისკის ნიშნები (სურათი 1, 2). ასეთი კვანძების ავთვისებიანობის რისკი 3%-ზე ნაკლებია და მასზე დაკვირვება ასევე შესაძლებელია ბიოფსიის გარეშე გაგრძელდეს. თუმცა, თუ კვანძის ზომა 2 სმ-ზე დიდია, აქ უკვე შეიძლება საჭირო გახდეს ბიოფსია.
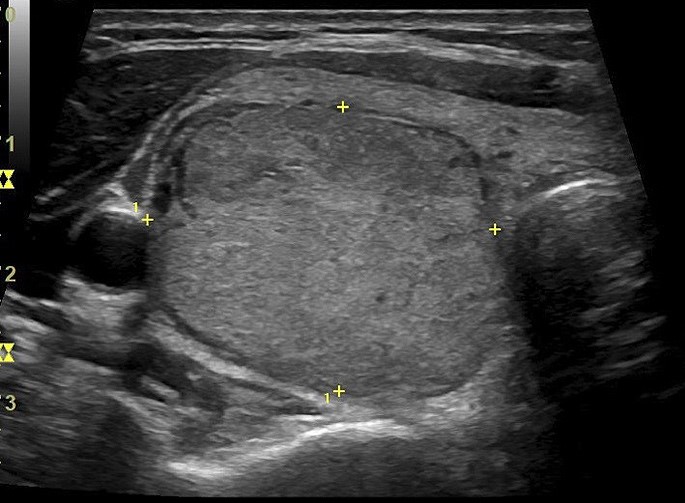
მცირე რისკის კატეგორიაში ხვდება ქსოვილოვანი შენების იზოექოგენური და ჰიპოექოგენური კვანძები, ასევე ნაწილობრივ ცისტური კვანძები ქსოვილოვანი არშიით, აქაც მაღალი რისკის ნიშნების გარეშე (სურათი 3). ასეთი კვანძების მალიგნიზაციის რისკი 5-10%-ია და ATA-ის რეკომენდაციით ბიოფსია უნდა ჩატარდეს, როცა ზომა 1,5 სმ-ზე მეტია.
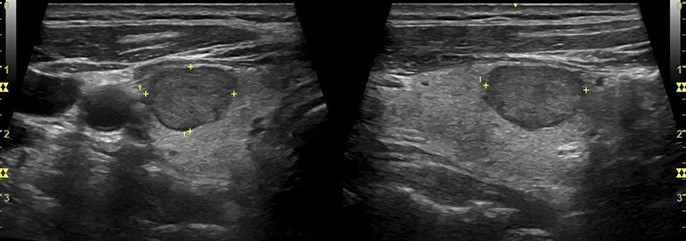
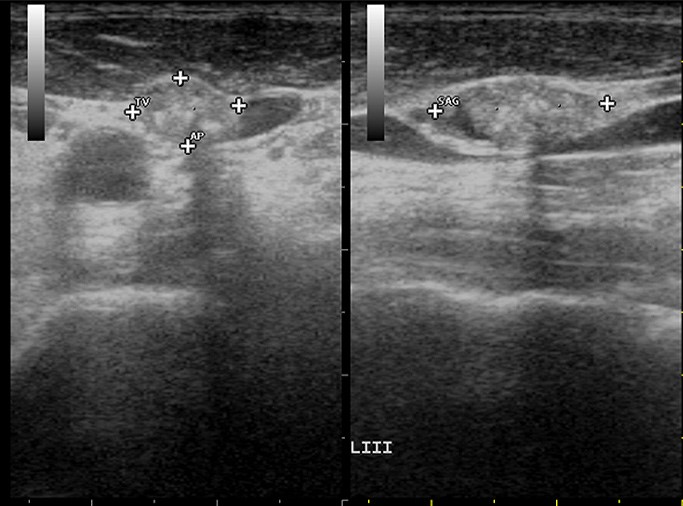
ზომიერი რისკის კატეგორიაში მოიაზრება ქსოვილოვანი ჰიპოექოგენური კვანძები მაღალი რისკის ნიშნების გარეშე. (სურათი 4). ამ შემთხვევაში მალიგნიზაციის რისკი 10-20%-ია და უნდა ჩატარდეს ბიოფსია, თუ ზომა 1 სმ-ზე მეტია.
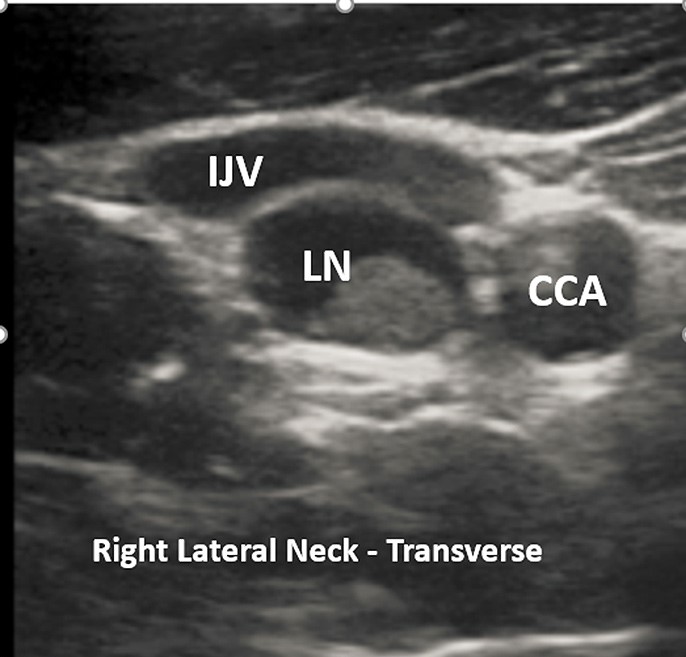
მაღალი რისკის კვანძების კატეგორიაში შედის სოლიდური ან ნაწილობრივ ცისტური შემადგენლობის კვანძები, რომელთაც აქვს შემდეგი მაღალი რისკის ნიშნები: არასწორი კონტურები, მიკროკალციფიკატები, უფრო მაღალი ვიდრე განიერი ფორმა, პერიფრიული რგოლისებრი კალციფიკაცია მცირე ექსტრუზიებით, ან ჯირკვლის გარეთ გავრცელების ნიშნები (სურათი 5,6). ამ დროს მალიგნიზაციის რისკი 70-90%-ია და ბიოფსია უნდა ჩატარდეს 1 სმ ზომის შემთხვევაში. ამავე კატეგორიაში შედის სონოგრაფიულად საეჭვო კისრის ლიმფური კვანძები (სურათი 7,8). ეს ხაზს უსვამს ფარისებრი ჯირკვლის ყოველი გამოკვლევის დროს ასევე კისრის წინა ნაწილის ლიმფური კვანძების გამოკვლევის აუცილებლობას.
თიროიდული ციტოპათოლოგია
ბეტესდას სისტემა თიროიდულ ციტოპათოლოგიას აჯგუფებს შემდეგნაირად:
- არადიაგნოსტირებადი
- კეთილთვისებიანი: კეთილთვისებიანი კვანძის დიაგნოზის დროს ავთვისებიანობის რისკი 0-3%მდეა. მისი მონიტორინგი შეიძლება გაგრძელდეს ულტრასონოგრაფიულად. თუ დინამიკაში დაფიქსირდება მაღალი რისკის ექოსკოპიური ნიშნების განვითარება, უნდა ჩატარდეს განმეორებითი ბიოფსია.
- განუსაზღვრელი მნიშვნელობის ატიპია/განუსაზღვრელი მნიშვნელობის ფოლიკულური დაზიანება
- ფოლიკულური ნეოპლაზია: ეს კატეგორია ატიპიასთან და ფოლიკულურ დაზიანებებთან ერთად მოიცავს დაუდგენელი ხასიათის კვანძებს, რომელთა ავთვისებიანობის რისკი 10-40%-ია. დიაგნოსტიკის მომდევნო ეტაპია ან მოლეკულური მარკერების ტესტირება ან დიაგნოსტიკური ლობექტომია.
- ავთვისებიანობაზე საეჭვო: ამ კატეგორიაში ავთვისებიანობის რისკი 45-60%-ია. რეკომენდაცია არის ქირურგიული ჩარევა: ლობექტომია ან ტოტალური თირეოიდექტომია.
- ავთვისებიანი: ეს დასკვნა 95-99%-ში მოიაზრებს ავთვისებიანი კვანძის არსებობას. რეკომენდაცია აქაც არის ქირურგიული ჩარევა ლობექტომიით ან ტოტალური თირეოიდექტომიით.
ACR TI-RADS გაიდლაინები იყენებს მალიგნიზაციის რისკის შეფასების ძირითადად იგივე სისტემას, რასაც ATA. ამ გაიდლაინში გადაწყვეტილების მიღებისას, ჩატარდეს კვანძის ბიოფსია, თუ მის გარეშე გაგრძელდეს მეთვალყურეობა, ულტრასონოგრაფიული მახასიათებლების და კვანძის ზომის გარდა, დამატებით ფაქტორად განიხილება ასევე ინფორმირებული პაციენტის არჩევანი, სხვა თანმხლები დაავადებების არსებობა და ასაკი.
როგორც თავად ულტრასონოგრაფიის ჩატარება, ასევე რისკის შეფასების სისტემის გამოყენება მნიშვნელოვნად ინდივიდუალურია და დამოკიდებულია ექიმზე, რომელიც აფასებს პაციენტს. რამდენადაც მკაცრი შეთანხმება კვანძების კატეგორიებთან მიკუთვნების მეთოდზე არ არსებობს, ექიმის პირად გამოცდილებას და მოსაზრებას დიდი მნიშვნელობა ენიჭება. არასაჭირო ბიოფსიების თავიდან ასაცილებლად და გამოსავლის გასაუმჯობესებლად მნიშვნელოვანია, რომ კვლევები ჩატარდეს სპეციალიზირებულ კლინიკაში საკუთრივ ფარისებრი ჯირკვლის კვლევაში გამოცდილების მქონე ექიმების მიერ.
წყარო: medscape.com




